



PRE-CONDITIONS THE OVARY FOR OVULATION INDUCTION
- DHEA supplementation for production of estrogen in the ovaries.
- Improves follicular dynamics enhances aromatase activity required for improved E2 levels.
- Better ovarian function in women with increased resistance to Ol increase no. of oocytes and embryos favoring clinical pregnancies.
REDUCES MISCARRIAGES RATES:
ABROSTERON-D supplementation has shown to have progestogenic effects in women with age related poor ovarian function to support conception and prevent miscarriages. It also augments gonadotrophin secretion that in turn augment HCG secretion to support corpus luteum for production of progesterone to support pregnancy Overall reduces miscarriages and improve cumulative pregnancy outcome.
IS THERE A ROLE IN PCOS? All patients with PCOS have increased sensitivity to androgens upto 70% have elevated androgen levels and other 30% are in the high normal range Hence initial conversion of DHEA to androgens does not favour its use in treatment of PCOS.
DOSAGE AND ADMINISTRATION: The recommended daily dose of DHEA is 25 mg in three divided doses till pregnancy and stop after pregnancy is confirmed. Administration of DHEA for two months 80 μg/day increased the level of DHEA to 544 ± μg. Administration of DHEA, four months prior to IVF cycles increases the response of ovaries to gonadotrophin treatment and improves the overall outcome.
WHY THREE MONTHS? It takes approximately 3 months for an immature egg to develop into a mature egg ready for ovulation, and this is the crucial window of opportunity to improve your egg quality. Whether you are trying to conceive naturally, through IVF or through a loss it is important that you do what you can to improve egg quality. You can become naturally pregnant at any point during supplementation, for IVF treatment we highly recommend at least three months supplementation to maximize your chances of a successful egg retrieval and healthy attachment.
ADVERSE REACTIONS: DHEA is unsafe when used in larger amount for prolonged period.
DRUG INTERACTIONS:
Anastrozole (Arimidex), Exemestane (Aromasin), Insulin, Letrozole (Femara)Some medications changed by the liver include loyastatin (Mevacor) etoconazole Nizoral), itrazonazole (Sporanox), Fexofenadine (Allegra), triazolam (Halcion), and many others., Medication for inflammation (Corticosteroids), decreases the effect of DHEA.
CONTRAINDICATIONS:
- DHEA supplementation is contraindicated in those with breast, uterine, prostate & ovarian malignancy Liver diseases, Pregnancy & breastfeeding Hormone-sensitive conditions such as breast cancer, uterine cancer, ovarian cancer, endometriosis, or uterine fibroids Diabetes Mood disorders Polycystic ovary syndrome
- Cholesterol problems. Side effects Acne Hair loss Stomach upset High blood pressure
- Some women can have changes in their menstrual cycle, facial hair growth, and a deeper voice after taking.
DHEA EVIDENCE-BASED STUDIES:
DHEA improve oocytes yield via IGF-1 They promote preanatal follicle growth by Granulosa cell specific androgen receptors ● Preventing follicular atresia ● Synergistic effect between DHEA and gonadotropins.
INSTRUCTIONS:
Store in a cool and dry place. Protect from light, heat and moisture. Keep out of the reach of children.
PRESENTATION:
Available in 30’s capsules Packing.
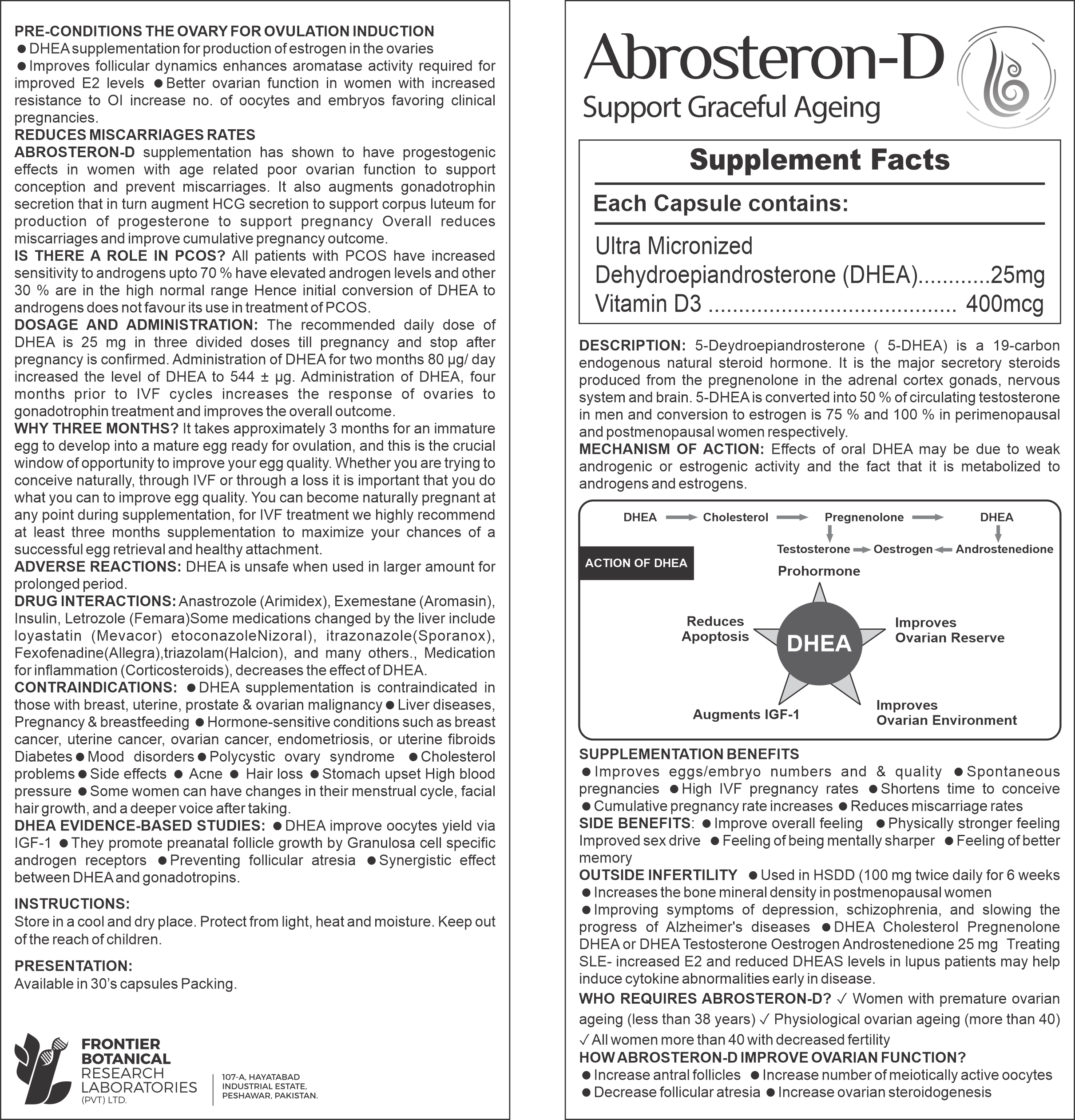
DESCRIPTION:
5-Deydroepiandrosterone ( 5-DHEA) is a 19-carbon endogenous natural steroid hormone. It is the major secretory steroids produced from the pregnenolone in the adrenal cortex gonads, nervous system and brain. 5-DHEA is converted into 50% of circulating testosterone in men and conversion to estrogen is 75 % and 100 % in perimenopausal and postmenopausal women respectively.
MECHANISM OF ACTION:
Effects of oral DHEA may be due to weak androgenic or estrogenic activity and the fact that it is metabolized to androgens and estrogens.
SUPPLEMENTATION BENEFITS
- Improves eggs/embryo numbers and & quality Spontaneous pregnancies .
- Improves Ovarian Environment.
- High IVF pregnancy rates Shortens time to conceive.
- Cumulative pregnancy rate increases Reduces miscarriage rates.
SIDE BENEFITS:
- Improve overall feeling
- Physically stronger feeling Improved sex drive
- Feeling of being mentally sharper
- Feeling of better memory
OUTSIDE INFERTILITY ⚫ Used in HSDD (100 mg twice daily for 6 weeks Increases the bone mineral density in postmenopausal women Improving symptoms of depression, schizophrenia, and slowing the progress of Alzheimer’s diseases DHEA Cholesterol Pregnenolone DHEA or DHEA Testosterone Oestrogen Androstenedione 25 mg Treating SLE- increased E2 and reduced DHEAS levels in lupus patients may help induce cytokine abnormalities early in disease.
WHO REQUIRES ABROSTERON-D?
- Women with premature ovarian ageing (less than 38 years)
- Physiological ovarian ageing (more than 40)
- All women more than 40 with decreased fertility
HOW ABROSTERON-D IMPROVE OVARIAN FUNCTION?
- Increase antral follicles
- Increase number of meiotically active oocytes
- Decrease follicular atresia
- Increase ovarian steroidogenesis



Reviews
There are no reviews yet.